
UNDERSTANDING YOUR MENSTRUAL CYCLE
Many women when you ask them would say,
“My cycle is 28 days,”
but when you ask them how they count it, you realise that what they are counting is not the menstrual cycle but the number of days they bleed.
That single misunderstanding is responsible for much of the confusion surrounding women’s reproductive health.
Most women have never been taught how to correctly count their cycle, interpret the changes occurring in their bodies, or recognise when something is normal and when it deserves medical attention. As a result, they often depend entirely on mobile apps, social media advice, or myths handed down from generation to generation.
Your body, however, is speaking to you every single day. The question is whether you understand its language.
The menstrual cycle begins on the first day of proper menstrual bleeding and ends the day before the first day of your next menstrual bleeding.
Day One is the day you experience actual menstrual flow, not the day you notice light brown spotting before your period begins, and certainly not the day your bleeding stops.
- If your period begins on July 1st and your next period starts on July 29th, your cycle is 28 days.
- If your next period begins on August 3rd, then your cycle is 33 days. It is really that simple.
One of the greatest complexities some women still believe is that every menstrual cycle should last exactly 28 days.
In reality, reproductive medicine has moved far beyond that idea.
For most healthy adult women, a cycle anywhere between about 24 and 38 days can still be considered normal, provided it remains relatively consistent from month to month.
A woman whose cycles are usually 26, 27 or 28 days is just as normal as another whose cycles are consistently 34 or 35 days. What concerns doctors is not simply the number of days but whether the pattern suddenly changes without explanation.
Another misconception is that every woman ovulates on Day 14. This is probably one of the most repeated statements in reproductive health, yet it is one of the least accurate.
👁️ Ovulation does not occur on a fixed calendar day for every woman.
A woman with a 35-day cycle is unlikely to ovulate on Day 14. Likewise, a woman with a 24-day cycle may ovulate much earlier.
Ovulation depends on the MATURATION OF THE OVARIAN FOLLICLE AND THE COMPLEX INTERACTION BETWEEN THE BRAIN, OVARIES AND HORMONES. Stress, illness, travel, poor sleep, excessive exercise, weight gain or loss, breastfeeding, thyroid disorders, Polyendocrine Metabolic Ovarian Syndrome (PMOS), some medications and approaching menopause can all shift the timing of ovulation.
This is why your body gives you better clues than your calendar.
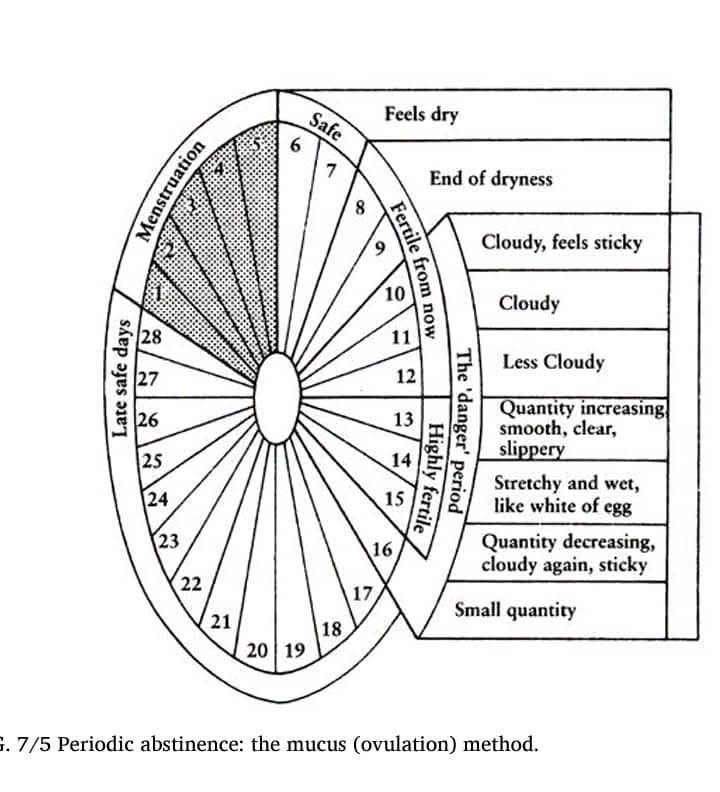
The image attached in comment section illustrates one of those clues, the changes in cervical mucus. Although it simplifies the process, it highlights an important biological principle.
Your cervix is not producing mucus randomly. The appearance, texture and amount of mucus change because your hormones are changing.
Immediately after menstruation, many women notice little or no discharge. The vagina may even feel dry. This usually reflects low estrogen levels and is generally regarded as a period of relatively low fertility.
Well, as estrogen gradually rises, the cervix begins producing thicker mucus.
At first it may feel sticky, tacky or pasty and often appears white or cloudy. As ovulation approaches, the mucus becomes creamier, resembling lotion or better said neat Aloe Vera gel. Fertility is increasing at this stage.
During the few days before ovulation, the mucus undergoes one of the most remarkable transformations in human biology. It becomes clear, slippery, stretchy and resembles raw egg white. This is highly fertile cervical mucus. It is not simply “discharge.” It is a sophisticated biological medium designed to protect sperm from the acidic environment of the vagina, nourish them, filter out abnormal sperm and help healthy sperm travel toward the egg. This is why pregnancy is most likely when this type of mucus is present.
After ovulation, progesterone becomes the dominant hormone. The cervical mucus quickly becomes thicker, stickier and much less abundant. Many women notice that the vagina feels dry again. This transition usually signals that ovulation has already occurred and fertility is declining.
However, not every vaginal discharge represents fertile cervical mucus. Many women mistake infections for normal discharge. Healthy cervical mucus should not produce a foul smell, severe itching, burning or pain. Green, grey or yellow discharge, frothy discharge, cottage cheese-like discharge or discharge associated with pelvic pain should never be ignored because these often suggest infection rather than fertility.
Your menstrual blood also tells a story.
Fresh menstrual blood is usually bright or dark red. Towards the end of menstruation it often becomes brown because the blood has remained in the uterus or vagina longer before leaving the body. This is generally normal.
Small blood clots may also occur, particularly on heavier days, because blood naturally coagulates before leaving the uterus. However, repeatedly passing very large clots, especially if they are accompanied by severe pain or excessive bleeding, should be medically evaluated.
Many women cannot accurately estimate how much blood they lose, so doctors often rely on practical descriptions rather than exact measurements. A normal menstrual period usually lasts between two and seven days. Bleeding that consistently lasts longer than seven days deserves further assessment.
Heavy menstrual bleeding is not simply “having a strong period.” If you soak through a pad or tampon every hour for two or more consecutive hours, need to change pads throughout the night because of flooding, regularly pass large clots, develop dizziness, shortness of breath or fatigue from blood loss, or become anaemic, this is not something to normalise. Heavy menstrual bleeding may result from fibroids, adenomyosis, endometriosis, hormonal imbalance, thyroid disease, bleeding disorders, certain medications, copper intrauterine devices, pregnancy-related complications or, less commonly, cancers affecting the uterus or cervix.
On the other hand, very light periods or absent menstruation are not always good news either. Pregnancy is the most obvious cause, but breastfeeding, excessive exercise, severe emotional stress, rapid weight loss, eating disorders, premature ovarian insufficiency, thyroid disease, elevated prolactin levels and Polyendocrine Metabolic Ovarian Syndrome (PMOS) can also suppress menstruation.
Many women also ask me what regular and irregular menstruation actually mean.
Regular menstruation does not mean your period arrives on exactly the same date every month.
A woman whose cycles are 27 days one month, 29 the next, then 28 and 30 days is still considered fairly regular because her body follows a predictable pattern.
Irregular menstruation refers to cycles that fluctuate widely without consistency. For example, having a 24-day cycle one month, a 38-day cycle the next, then 29 days followed by 46 days may indicate that ovulation is not occurring consistently or that an underlying medical condition requires investigation.
Pain deserves attention too.
Although mild menstrual cramps are common because of prostaglandins that help the uterus contract, pain so severe that it prevents you from going to school, working, walking or carrying out normal activities should never be dismissed as “part of being a woman.” Conditions such as endometriosis and adenomyosis frequently go undiagnosed because women are told to simply tolerate the pain.
Bleeding between periods, bleeding after sexual intercourse, persistent pelvic pain, foul-smelling discharge, fever, sudden changes in menstrual pattern after years of regular cycles, or the complete absence of menstruation for several months in a non-pregnant woman should all prompt medical evaluation.
Perhaps the greatest mistake women make today is relying entirely on period-tracking applications without observing their own bodies.
Apps predict your cycle based on averages. Your ovaries do not follow algorithms. Your hormones respond to stress, nutrition, sleep, illness, medications, body weight, exercise, age and dozens of other biological variables. Learning to observe your cervical mucus, menstrual flow, symptoms, basal body temperature where appropriate, and overall cycle pattern provides a much more accurate understanding of your reproductive health.
Your menstrual cycle is far more than a monthly inconvenience. It is one of the most valuable health indicators you possess.
Every cycle tells a story. The colour of your blood, the amount you bleed, the presence or absence of pain, the changes in your cervical mucus, the regularity of your periods and even the timing of ovulation are all messages from your body.
The more you learn to understand those messages, the earlier you can recognise potential problems, preserve your fertility, protect your reproductive health and make informed decisions about your wellbeing. Knowledge of your menstrual cycle is not merely about pregnancy or contraception; it is about understanding yourself as a woman.







